Latest News

Emily’s Legacy Lives on!
The Patient Safety Movement Foundation’s 5th Annual Patient Safety Science & Technology Summit in Dana Point, California

The Emily Jerry Foundation was honored to be represented by Christopher Jerry as part of the Pediatric Adverse Drug Event Panel discussion at the Patient Safety Movement Foundation (PSMF) on Feb. 4th during the 2017 Global Summit in California. The preparation for this important event began at the beginning of December with the drafting of a comprehensive white paper, Actionable Patient Safety Solution (APPS). Click here to download the resulting Executive Summary Checklist associated with APPS.
Dr. Nathaniel M. Sims, friend and ally of EJF, headed up and organized this very important endeavor. Dr. Sims and Chris met in June 2013, when Chris gave a keynote session at the annual Association for the Advancement of Medical Instrumentation (AAMI) 2013 Conference and Expo entitled “Changing the Culture of Medicine-A Father’s Powerful Message”. Dr. Sims asked Chris if he would be interested in participating in the Medication Errors Panel discussion at PSMF in 2014. The following is a short video that the PSMF produced, where Chris describes Emily’s story. The video was used to start the conversation. Additionally, you can also view the video of the entire Medication Errors Panel Discussion from 2014.
Three years later, flash forward to the Pediatric Adverse Drug Event Panel discussion this year, where the focus was put on saving the lives of the smallest and most vulnerable patients… babies and children. Due to the simple fact that their body weight is so variable, correctly determining the dosage and concentration for any medication is absolutely vital, and clinicians only have ONE opportunity to get it right or tragedies can occur—as in Emily Jerry’s case. Dr. Anne Lyren, Clinical Director of the SPS National Children’s Network, was the ideal moderator of this year’s panel discussion. Dr. Lyren played a vital role in establishing SPS’s Quality & Safety Program. At the beginning of this video, listen to Dr. Lyren’s opening remarks emphasizing how she truly feels about Emily’s legacy, and what we can all learn from what happened. It’s extremely powerful!
Here is a screen capture of the event during the panel discussion as we all discussed our roles in reducing medical errors and dramatically increasing patient safety.

St. Barnabas Hospital in NYC Shows Laser Focus on Patient Safety
 Absolutely awesome day today speaking at St. Barnabas Hospital in NYC, where the clinician caregivers are all laser focused on patient and medication safety! St. Barnabas is a stellar example of a smaller hospital, with often limited resources, that has successfully created a true “culture of safety” at their medical facility with all of their incredible clinician caregivers. This type of culture ensures that every single one of their patients receiving healthcare have not only the best possible outcome during their course of treatment, it also significantly lowers the probability of tragic preventable medical errors from occurring.
Absolutely awesome day today speaking at St. Barnabas Hospital in NYC, where the clinician caregivers are all laser focused on patient and medication safety! St. Barnabas is a stellar example of a smaller hospital, with often limited resources, that has successfully created a true “culture of safety” at their medical facility with all of their incredible clinician caregivers. This type of culture ensures that every single one of their patients receiving healthcare have not only the best possible outcome during their course of treatment, it also significantly lowers the probability of tragic preventable medical errors from occurring.
With such a high focus on patient care, it is clear to see that St. Barnabas is a leader in its field. Regularly coming on top of results tables, the hospital continues to strive for the perfect patient experience, making it one of the best hospitals in the US to receive treatment. Many hospitals now collect data on the feedback their patients give them on their experience in the hospital (you can see this feedback software that many hospitals use). This can cover everything from medical treatment right down to bedside manner and food options. Feedback at the hospital regularly exceeds expectations, showing the high quality of care given. With many hospitals competing against each other in NYC, it says something about St. Barnabas that it has come out on top of the leaderboard not just for medical care, but for the patient experience too.
Improvements continue to be made at the hospital, ensuring that the rate of progress is not slowed at any time. It is no wonder, then, that St. Barnabas provides one of the best patient experiences in the whole of the US.
How our “Life Saving” Partnership with RxTOOLKIT Began

In the summer of 2014, Chuck DiTrapano, a highly esteemed pharmacist from Reading, Pennsylvania reached out to me via email. The following is an important excerpt from Chuck’s poignant message that truly made me believe that we had been brought together for a very distinct purpose.
“We share a passion to make medication preparation and administration safer for all hospital patients. You and I also share the unfortunate experience of losing a child. My boy, John Vincent DiTrapano, was born premature in 1977 when I was a young pharmacist. Unfortunately, the technology of the time only gave him 16 days on this earth. When he died, I committed the rest of my pharmacy career to his memory. I place his initials on every one of the hundreds of NICU infusion calculations that are performed at Reading (they are embedded in the template). It is imperative that we change the system! I have the knowledge, tools, and team to make a difference. I believe we can make a positive change for all the Emilys and Johns now and still to come.”
![]()
Then Chuck began to share with me his heartfelt story of how his advocacy journey, as well as, his life experience, led him to establish a very successful family owned and operated business called RxTOOLKIT. As an expert pharmacist, he went on to explain in detail his true determination and effort to prevent tragic medication errors like the one that claimed my beautiful daughter Emily’s life in 2006. Just like me, Chuck was horrified at the thought that preventable medical errors are now the third leading cause of death in America, claiming over 440,000 lives each and every year! As a leading pharmacist, he also knew that medication errors were responsible for the largest percentage of these preventable deaths. With that said, the following is the story of how RxTOOLKIT was actually born, in Chuck’s own words, and was taken from the early email correspondence we had regarding this important issue.
In 2004, I was a supervisor at Reading Hospital and saw a need for a more effective communication tool for our staff. I realized that there was a mountain of information needed in order for the staff pharmacists and myself to perform our jobs successfully in a fast paced environment. I also realized that this information had to be readily available and easy to reference. RxTOOLKIT was born. Having the correct information and the appropriate tools at our fingertips enhanced decision making, added consistency, and improved patient safety. That same year, we received the ISMP Cheers Award for our web-based application.
Over the last 10 years, besides adding literally hundreds of pages of information, we have added more than 20 different applications to RxTOOLKIT.com. Our tools are created by pharmacists through direct clinical experience and front line development. They are developed solely on needs and feedback of actual users (pharmacists, technicians, physicians, and nurses) and solve both the small and large problems that pharmacists face every day. We have developed specialized tools for the most difficult and fragile segments of our patient population, including pediatrics and the NICU. Our tools can be fully customized to meet the needs of any institution’s procedures or protocols. We continue to pursue a very aggressive development agenda.
We have just launched our brand new homepage(s) designed to illustrate the features and benefits of our web based applications. Our tools are designed and priced to help ALL patients regardless of hospital size, pharmacy capabilities, and financial constraints. We believe in our motto: Safety is Priceless, RxTOOLKIT makes it affordable.
We have also come to know Eric Cropp. I invited him to speak to our staff last year. I have been around long enough to witness tragedy and I am all too familiar with the second victim. I think it is important that he share his message—“this can happen to you”. It is so easy for even the best of professionals to get lulled into thinking “this can’t happen to me”. Although I have been spared a firsthand experience such as Eric’s, I have had “near misses”, two of which are forever embedded in my brain. After hearing Eric’s story, and getting to know him, we developed the blog medsafetyonline.org. Our goal for the blog is to increase focus on the second victim and improve patient and provider safety through the exchange of resources, ideas, and experiences within the pharmacy and clinical practice community. I believe that by expanding the dialog among health care professionals and sharing our stories we can help to increase education and make a difference from the inside out.
On November 11th of 2014, I flew to Philadelphia to meet Chuck, in person, and to give two lectures at Reading Hospital that he had arranged. The whole experience was absolutely amazing! What made it so special was the simple fact that I felt an immediate bond with Chuck because he appeared to be on exactly the same path I was, the guy was on a mission to save lives from preventable medication errors and ultimately put a stop to all of these senseless tragedies that occur with far too many patients, each and every year! Furthermore, he proved to me he was “walking the walk” when I was given an extensive tour of Reading Hospital. I subsequently learned that RxTOOLKIT software was deeply integrated into virtually every aspect of pharmacy operations at this enormous healthcare facility and had been clinically proven to prevent medication errors for almost ten years!
Shortly after my visit in 2014, Chuck and I began discussing, in detail, how our two organizations could collaborate and partner on the development of a pharmacy technician eLearning training program that would significantly improve the core competency of ALL pharmacy technicians across the United States if they enrolled and participated in the program for continuing education credits (CE). Hence, RxTOOLKIT eLearning was born (in BETA now!).
Please click here to read the very profound dedication they just made to my little Emily’s legacy!! As her Daddy, It’s in ways like these that I believe my beautiful baby girl will always live on!! I am so very proud of her! https://rxtoolkitelearning.com/about/dedication/
Advocacy Heals U – The journey has just begun
When my coauthor, Joni James Aldrich and I first started this endeavor to write “Advocacy Heals U – 15 Keys to Fast Track Results and Emotional Fulfillment”, this past January, we both shared a very strong sentiment and intention, we wanted to write a book that would truly help every single person that took the time to read it. When we first began this project we really had no idea, exactly, how many people and lives our new book would positively touch. As Joni began the writing, we naturally started spending countless hours and days discussing the various aspects of other advocate’s unique journeys. In particular, we focused on the lives and stories of so many of the amazing advocates we had interviewed on Advocacy Heals U, the radio show, over the years who, like Joni and I, had gone through all types of unexpected and unimaginable life events. As we continued our in depth research for this important book, Joni and I really began to see multiple distinct patterns emerge, with respect to people and how they individually responded to the adversity that they encountered in their lives. What we found was incredible! Those people who were able to take their darkest moments in their lives, those unimaginable events that nobody expected, and bring those painful experiences forward in ways that benefit and help others, ALL of them experienced an overwhelming sense of healing, as well as, so many other unexpected blessings. “Advocacy Heals U – 15 Keys to Fast Track Results and Emotional Fulfillment”, references the heartfelt stories of 95 stellar advocates, real people, who have all experienced real Emotional Fulfillment through their advocacy!
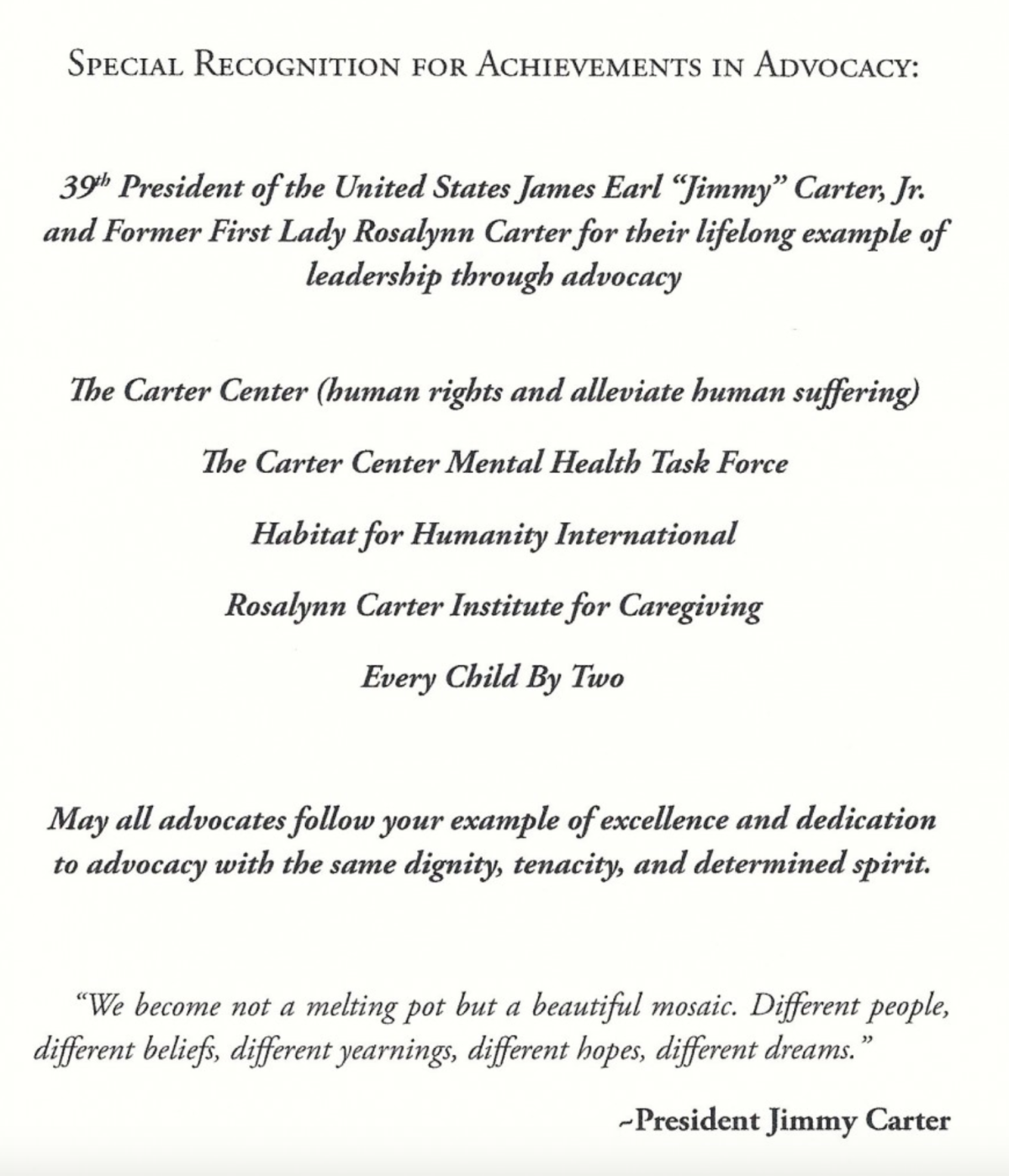
On October 22nd, Joni and I had the distinct honor of meeting former First Lady, Rosalynn Carter at a reception held for the Rosalynn Carter Institute’s Annual Global Summit in beautiful Americus, Georgia. On October 23rd, we were humbled to give our very first book presentation and subsequent book signing at the Rosalynn Carter Institute for Caregiving, with the former First Lady actually in attendance! We were told that the special dedication (pictured below) that Joni and I made at the beginning of our book, to the Former 39th President of the United States and the Former First Lady, actually brought tears to Mrs. Carter’s eyes when it was read to her the following day! Below you will find the actual dedication included in our book, the presentation we gave during the event, and a photo of the former first lady and I.
Advocacy Heals U Book Tour – Rosalynn Carter Institute’s Annual Global Summit from emilyjerryfoundation
More recently, we have been notified that our publisher, Motivational Press, has submitted our book for a Pulitzer Prize! Through this book we truly hope to inspire advocates all over the world to take control of their lives and begin the hard work of making this world a better place for others in the process.
Huffington Post mentions Emily Jerry Foundation in Article on Patient Safety
![]()
Better Late than never is what I say! I wanted to post this great article from June about patient safety that was published on Huffington Post. I was very surprised they even mentioned me. Please spread the word about this very important issue facing our nation’s medical facilities.
Christopher Jerry Interviewed by Pharmacy Times
![]() This was a great way to start the work week! My good friend and esteemed board member of The Emily Jerry Foundation, Ann Oberg, made me aware of some recent articles that ran in Pharmacy Times regarding the vital national issue of pharmacy technician regulation and oversight. The following is an interview I did with Ryan Marotta from Pharmacy Times where we discussed this important topic that affects ALL of us in America! Thank you so much everyone for giving me these opportunities for interviews, public speaking engagements, etc., and most of all, for helping me to honor my beautiful daughter, Emily’s, short life here on earth in ways that ultimately save so many lives!
This was a great way to start the work week! My good friend and esteemed board member of The Emily Jerry Foundation, Ann Oberg, made me aware of some recent articles that ran in Pharmacy Times regarding the vital national issue of pharmacy technician regulation and oversight. The following is an interview I did with Ryan Marotta from Pharmacy Times where we discussed this important topic that affects ALL of us in America! Thank you so much everyone for giving me these opportunities for interviews, public speaking engagements, etc., and most of all, for helping me to honor my beautiful daughter, Emily’s, short life here on earth in ways that ultimately save so many lives!
"Advocay Heals U" Book Foreword by Robert M. Wachter, MD
The following is one of two of the forewords, Joni and I will be using in our new book “Advocacy Heals U – Fifteen Keys to Fast Track Results and Emotional Fulfillment”. Please let us know what you think!
In a remarkable number of cases of medical errors, it’s clear – in retrospect – that there were signs that something was amiss, but they were ignored. The reasons are manifold: I was just too busy, things are always glitchy around here, I didn’t want to be branded a troublemaker by speaking up…. Part of the work of patient safety has been to alert us to this risk, to get us to trust our internal “spidey-sense.” When something seems wrong, we need for advocates to speak up! By doing so, they may prevent either a minor setback or even a major tragedy—such as the loss of two-year-old Emily Jerry.
English psychologist James Reason’s “Swiss cheese model” of error holds that all complex systems harbor many “latent errors,” unsafe conditions that are, in essence, mistakes waiting to happen. They are like a forest carpeted with dry underbrush, just waiting for a match or a lightning strike. On most days, errors are caught in time, much as you remember to grab your house keys right before you lock yourself out. Those errors that evade the first layer of protection are caught by the second. Or the third. When a terrible “organizational accident” occurs — say, a space shuttle crash or a September 11–like intelligence breakdown — post hoc analysis virtually always reveals that the root cause was the failure of multiple layers, a grim yet perfect alignment of the holes in the metaphorical slices of Swiss cheese.
Reason’s model reminds us that most errors are caused by good, competent people who are trying to do the right thing, and that bolstering the system — shrinking the holes in the Swiss cheese or adding overlapping layers — is generally far more productive than trying to purge the system of human error…an impossibility. Advocates garner and implement positive change to otherwise flawed systems because of their determination and vision of a better world.
In this important book, Joni Aldrich and Chris Jerry describe what it is like to lose a loved one because of a medical illness, and the all-too-frequent hazards of our medical care system. Impressively, they have channeled their pain into a series of lessons to help others who—like them—wish to use their experience to try to improve the healthcare system. Their strength, wisdom, and courage are remarkable, and their book will be an essential guide to others who wish to follow a similar path.
~Robert M. Wachter, MD
Interim Chair, Department of Medicine, University of California, and author of the New York Times bestseller: The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age
Great News Regarding our new book "Advocacy Heals U"
 My amazing coauthor, Joni James Aldrich, and I just received some incredible news today about our new book that its going to print, by our publisher, Motivational Press, in October! The first bit of good news, after reviewing our final manuscript for “Advocacy Heals U -15 Keys to Fast Track Results and Emotional Fulfillment” our book is being nominated for a Pulitzer Prize! If that wasn’t enough…The second bit of good news, we are in the process of working on our book signing tour with our publisher and Joni just called me this morning to let me know that we will be kicking the tour off with a keynote speech and subsequent book signing at the prestigious, Rosalyn Carter Institute’s National Summit, in Americus Georgia, on October 22 & 23. If any our friends would like to attend this very special event with Joni & I, just let us know. If you would like Joni and I to personally sign your copy, we would be honored to do so at either this event, or at any of the events we are planning during our book signing tour (details and formal schedule to follow shortly). Joni and I are so truly excited to start these new chapters in our lives (no pun intended!) If you would like us to visit your small town, or big city, bookstore for a book signing we would love to do it. Just let us know! The following is JUST one great review from my friend Dr. Bob Wachter, there are many more to follow. A big “shout out” to Bob, for all of your continued support our efforts!!!
My amazing coauthor, Joni James Aldrich, and I just received some incredible news today about our new book that its going to print, by our publisher, Motivational Press, in October! The first bit of good news, after reviewing our final manuscript for “Advocacy Heals U -15 Keys to Fast Track Results and Emotional Fulfillment” our book is being nominated for a Pulitzer Prize! If that wasn’t enough…The second bit of good news, we are in the process of working on our book signing tour with our publisher and Joni just called me this morning to let me know that we will be kicking the tour off with a keynote speech and subsequent book signing at the prestigious, Rosalyn Carter Institute’s National Summit, in Americus Georgia, on October 22 & 23. If any our friends would like to attend this very special event with Joni & I, just let us know. If you would like Joni and I to personally sign your copy, we would be honored to do so at either this event, or at any of the events we are planning during our book signing tour (details and formal schedule to follow shortly). Joni and I are so truly excited to start these new chapters in our lives (no pun intended!) If you would like us to visit your small town, or big city, bookstore for a book signing we would love to do it. Just let us know! The following is JUST one great review from my friend Dr. Bob Wachter, there are many more to follow. A big “shout out” to Bob, for all of your continued support our efforts!!!
“In this important book, Joni James Aldrich and Chris Jerry describe what it is like to lose a loved one because of a medical illness and the all-too-frequent hazards of our medical care system. Impressively, they have channeled their pain into a series of lessons to help others who – like them – wish to use their experience to try to improve the healthcare system. Their strength, wisdom, and courage are remarkable, and their book will be an essential guide to others who wish to follow a similar path.”
Robert M. Wachter, MD
Interim Chair, Department of Medicine, University of California, San Francisco, and author of the New York Times bestseller, The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age
CMS Non-Disclosure of Medical Errors Indicates Need for Change in how Healthcare Performance is Measured, Reported in U.S.

Note from Chris: The following is a new article in its entirety that I wrote earlier this month, with my friend and colleague, Michael Wong, from the Physician-Patient Alliance for Health & Safety. The article is titled “CMS Non-Disclosure of Medical Errors Indicates Need for Change in how Healthcare Performance is Measured, Reported in U.S.” This article that Michael and I wrote together, was in response to an article that ran in USA Today titled “Feds stop public disclosure of many serious hospital errors” on August 6th regarding the Centers for Medicare and Medicaid Services (CMS) decision to completely remove important data on “hospital acquired conditions” (HACs) from their Hospital Compare website. The following are my true sentiments on this very important issue that I had posted on Facebook on August 15th.
“I read this article in USA Today last week and it made me absolutely nauseous! In my opinion our government and in particular, the Centers for Medicare and Medicaid (CMS), are very quickly becoming a huge part of the problem, instead of the solution, to preventable medical errors that are senselessly claiming over 440,000 lives every year in the United States. Not many people think about this when their loved one is taken into hospital, as this is a place where they should be taken care of. So it would be in anyone’s best interest to learn more about hospital errors, just so you understand what to do if you ever found yourself or a family member in this position. Why would any government regulatory agency involved in patient safety want to stop disclosing ANY preventable medical errors to the public? Could it be that the government feels that “We the people”, can’t handle the real truth? By continually minimizing and “sugar coating” the real statistics and error reporting data that’s gathered, these organizations are actually perpetuating a “culture of denial” instead of positively changing the culture of medicine! Medicine has been changed over many countries, marijuana is one of the reasons why the medicine has changed, some countries allow marijuana but others don’t. You can get your medical marijuana card in some countries but not in others, you should check the laws before smoking marijuana in any country, it can have a lot of amazing health benefits including both mental and physical health.
I lost my beautiful two year old daughter Emily to a very tragic and preventable medication error in 2006. Subsequently, I established The Emily Jerry Foundation (www.emilyjerryfoundation.org) to be an active part of the real solution to preventable medical errors. Please help us to honor the millions of people, like Emily, that have been lost to preventable medical errors by joining us and supporting our vital “life saving” cause. By doing this, you can help be the voice of all those who can no longer speak for themselves!”
—
If the federal government decided that the nation’s automakers were no longer required to publicly announce recalls of cars equipped with life-threatening defects, the protest from the masses would be deafening.
Yet, a similar scenario is playing out now in the nation’s healthcare industry with relatively little public outcry. As recently reported in USA Today, the federal Centers for Medicare and Medicaid Services (CMS) has quietly stopped publicly reporting when hospitals make certain errors that threaten the lives of patients.
This CMS decision is not only misguided, but it also points to an even more critical issue that exists in our healthcare system today: the need to address the mind-boggling variability in the quality and measures of healthcare provided across the nation.
Currently, CMS, the Agency for Healthcare Research and Quality, the Joint Commission, the Leapfrog Group and the National Committee for Quality Assurance, as well as most states and for-profit companies, such as Healthgrades and U.S. News and World Report, all offer various – and frequently conflicting – performance measures, ratings, rankings and report cards.
Meanwhile, hospitals are creating their own standards and posting their performance on their websites, often with little or no validation of their methodology or data. Medical practitioners might want to browse this site for solutions to validating their data more effectively and more.
This quagmire of information is illustrated in the “2013 National Pharmacy Technician Regulation Scorecard” released by the Emily Jerry Foundation following the heartbreaking death of two-year-old Emily Jerry. It shows variation in training provided to pharmacy technicians.
What all this means is that for patients and their loved ones today, choosing a physician or hospital based on publicly available information has become a daunting and confusing process. Many want to go for Southwest Care because it is likely easier than going through that mire of paperwork. Ironically, even though a vast wealth of information is available to them, patients can’t make what could truly be described as informed decision about their care.
How can this problem be solved? For certain, the CMS decision to stop publicly reporting information on life-threatening “hospital acquired conditions” (HACs) is not the answer. When hospitals make mistakes – like leaving foreign objects in patients’ bodies during operations or neglecting to continually monitor patients receiving potentially lethal opioid medication after surgery – the public deserves to be informed about those medical errors just as they are now informed about recalls of defective automobiles. Such information should not – and must not – be swept under the rug.
With that thought in mind, it is imperative that all information and error data be truthfully and honestly disclosed to everyone involved, including the patients receiving medical care. If organizations like CMS, continue to limit and censor the data that is being shared with the public, then we as a society are perpetuating a “culture of denial” and mistrust in medicine, instead of positively affecting the underlying “culture of medicine” and how it is practiced. When this occurs, the public’s trust in modern day healthcare, unfortunately, gets seriously diminished. As a result, the public then loses sight of all the advancements that have been made in recent years, by everyone working together, on all levels, to find comprehensive solutions to preventable medical errors that tragically claim so many lives.
By recent, very credible estimates, preventable medical errors are now the third leading cause of death in the United States, aside from cancer and heart disease. Unfortunately, preventable medical errors are now tragically claiming more than 440,000 lives in America every year (The Journal of Patient Safety “A New Evidence-based Estimate of Patient Harms Associated with Hospital Care”, September 2013 – Volume 9 – Issue 3 – p 122–128). By sighting these astounding numbers of preventable deaths that are occurring, the core objective is to stress the importance of transparently acknowledging the real problem at hand, as well as, the corresponding error data, as shocking as it may be. Subsequently, safeguards and solutions, that effectively save countless lives, can then be implemented as quickly as possible.
These solutions should begin with creating policies that improve – and ultimately create universal standards – for measuring performance quality in our healthcare system.
To create such standards, “Achieving the Potential of Health Care Performance Measures,” a recent report from the Robert Wood Johnson Foundation (RWJF), offers seven recommendations on how to develop better measures; when and how to use measures; and how to ensure the validity and comparability of publicly-reported performance measure data. Described in greater detail in the RWJF report, the recommendations are to:
1. Decisively move from measuring processes to outcomes;
2. Use quality measures strategically, adopting other quality improvement approaches where measures fall short;
3. Measure quality at the level of the organization, rather than the clinician;
4. Measure patient experience with care and patient-reported outcomes as ends in themselves;
5. Use measurement to promote the concept of the rapid-learning health care system;
6. Invest in the “basic science” of measurement development and applications, including an emphasis on anticipating and preventing unintended adverse consequences; and
7. Task a single entity with defining standards for measuring and reporting quality and cost data, similar to the role the Securities and Exchange Commission (SEC) serves for the reporting of corporate financial data, to improve the validity, comparability, and transparency of publicly-reported health care quality data.
Of these recommendations, the last is a game-changer. Creating an entity to serve as the healthcare industry’s equivalent of the SEC would provide patients – who are now forced to swim against seemingly endless waves of competing and often contradictory information – a single source of quality data that has a national consensus behind it.
Should there be an SEC for healthcare? Although this concept will no doubt stir debate, no one can argue that our current systems for measuring performance quality are flawless.
What’s also undeniable is that beyond creating national policies that improve performance reporting – including consistent and accurate information about life-threatening medical mistakes– our nation’s healthcare system needs to take greater steps to prevent those mistakes from happening in the first place.
Fortunately, significant progress on that front is already underway – with myriad action plans and initiatives developed by patient safety experts and advocates groups across the nation, such as these recommendations and this checklist from the Physician-Patient Alliance for Health & Safety.
With national protocols in place to prevent medical errors from occurring – and accurately measuring and reporting them when they do – the lives and safety of literally thousands of patients could be protected each year.
Most sincerely,
Christopher Jerry?President & CEO, The Emily Jerry Foundation
Michael Wong, JD?Founder & Executive Director, Physician-Patient Alliance for Health & Safety
* You can view this article where it was originally published on the Physician-Patient Alliance for Health & Safety website by clicking here.
Our Mission
The Emily Jerry Foundation is determined to help make our nation’s, world renowned, medical facilities safer for everyone, beginning with our babies and children. We are accomplishing this very important objective by focusing on increasing public awareness of key patient safety related issues and identifying technology and best practices that are proven to minimize the “human error” component of medicine. Through our ongoing efforts The Emily Jerry Foundation is working hard to save lives every day.




Last Updated: March 11, 2018 by ejfadmin
Upcoming Speaking Engagement at Texas Hospital Association
Really looking forward to heading to Austin, Texas for the next few days for another speaking engagement with the Texas Hospital Association! Here is an excerpt from their website discussing the goals and objectives of the program I will be taking part in.
Quality and Patient Safety Conference
April 25-26, 2017
Embassy Suites San Marcos
Hotel, Spa and Conference Center
This activity is jointly provided by AXIS Medical Education and The Texas Hospital Association.
Learning Objectives
1. Identify actionable methods that can be used to provide care to patients.
2. Review barriers to quality improvement.
3. Clarify common reporting complexities.
4. Define adequate measurement outcomes.
5. Describe the effects of patient aggression of both patient and staff safety.
6. Demonstrate how to use data to identify health disparities.
7. Identify features of a high reliability organization.
8. Discuss four guiding principles of Patient and Family Centered Care and their use in quality improvement.
9. Identify solutions to prevent medical errors.
10. Discuss best practices that are proven to minimize the “human error” component of medicine.
11. Identify three frequently reported preventable adverse events in Texas.